A Need for New Standards
Downsize Routine Adult ETTs and Check Cuff Pressure.
Introduction:
General anesthesia with an endotracheal tube (ETT) is performed safely countless times every day with an estimated anesthetic complication rate between 0.0606 to 0.0905 occurrences per 1,000 surgical discharges.1 Post-operative sore throat (POST) and post-operative hoarseness (PH), however, remain a common complaint of intubated patients with an estimated incidence of between 14-70%.2 High endotracheal tube cuff pressure and large size ETTs have been implicated as causative factors. These two factors have also been implicated in the catastrophic complications of tracheal stenosis and recurrent laryngeal injuries.3,4 The simple method of regulating cuff pressure with a cuff manometer and the use of smaller endotracheal tubes could limit these complications.
Literature Review:
In a thesis study by Evans 5 three different means of inflating the ETT pilot balloon were compared: the injection and palpation method, the minimum occlusive technique and the set volume of air. Forty-six percent of the ETT cuffs were inflated using the pilot balloon palpation technique, 28% using the set volume technique and 26% using the minimum occlusive technique. Regardless of the technique, none of the cuff pressures was within the acceptable range of 20-30 cm H2O. pressure. Thirteen percent of cuff pressures were below the minimum value necessary to prevent aspiration and 87% were inflated above the accepted value, risking tracheal ischemia.
In a study by Liu (2010), 509 patients from 4 university hospitals requiring general anesthesia with an endotracheal tube were studied to investigate the short-term (hours) impact of endotracheal intubation and cuff pressure. They were divided into two groups: control group did not measure cuff pressure and the study group had the ETTc measured. Additionally, 20 patients whose duration of anesthesia was between 120 and 180 minutes were selected from each group for fiberoptic bronchoscopy immediately after extubation. There was no significant difference in sex, age, height, weight or procedural length. The mean endotracheal tube cuff (ETTc) pressure measured after manual palpation was 43 +/- 23.3 mmHg with the highest at 210 mmHg. The incidence of post procedural sore throat, hoarseness and blood-streaked expectoration in the control group was significantly higher than in the study group. Fiberoptic bronchoscopy in the 20 previous selected patients from each group showed that the tracheal mucosa was injured in varying degrees but the injury was more severe in the control group. The authors suggest ETTc pressure monitoring and controlling in reducing complications.6
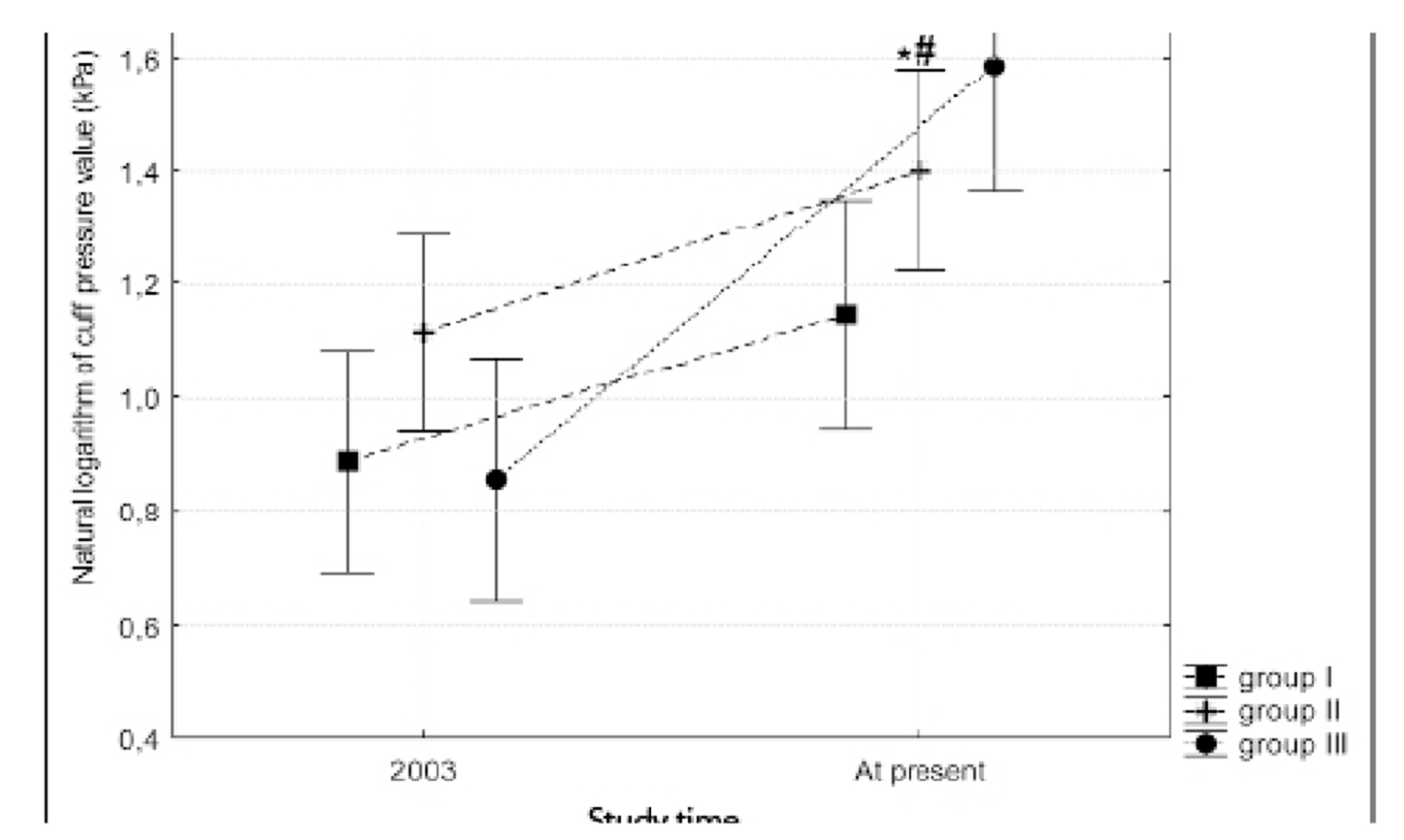
Wujtewicz (2009) analyzed ETT cuff pressure on the basis of the aneaesthesiolgist’s experience. Results were compared to those obtained during a previous study that was done in 2002. The physicians were divided into three groups according to experience: group 1 – less than 2 years of practice, group II – 2-10 years of practice and group III – over 10 years practice. He found a “tendency toward over-inflation of endotracheal tube cuffs with the problem more common in highly experienced anesthesiologists.” He also found “over-inflation was more prevalent in 2009 than in 2002”.7 The graph below is the data from Wujtewicz comparing 2002 to 2009:
Curiel8 studied forty patients who required endotracheal intubation for elected surgery. Patients who had ETT cuff pressures equal or less that 42 mmHg were assigned to group A, and those with higher than 42 mmHg to group B. Tracheal pain was assessed at 60 minutes and 24 hours after extubation. The tracheal pain was similar at 60 minutes after extubation but at 24 hours persisted only in 10% of subjects in group A and 53.3% of the subjects in group B, p=0.00001. The authors concluded that there is a need for routine monitoring of cuff pressure to avoid pressures that exceeds the appropriate range of 20-30 mmHg.
In a study by Galinski9 that measured the ETTc pressures of 107 patients intubated either by emergency out-of-hospital medical teams or transferred patients. Eighty-eight of the patients were intubated out-of-hospital and twenty-two were transfers between hospitals. The authors found 79% to be greater than 27 cm H2O with a mean pressure of 56 cm (SD+/- 34 cm H2O) for the out-of–hospital patients and a mean pressure of 69 cm H2O (SD+/- 37 cm H2O) for the
transferred patients.
In a study from 2012, researchers measured the cuff pressure of 136 patients in the operating room. Most of the pressures fell outside safe limits of 20-30 cm H2O. The minimum cuff pressure was 1 cm H2O to a maximum of 120 with a mean of 38 and SD of 31.
The problem of improper cuff inflation is not new. In 1988, Koay11 studied 200 patients undergoing general surgery with an endotracheal tube. The patients were divided into 2 groups. The first group (control) had the pilot balloons inflated with 5 cc of air. There was no record of intra-cuff pressure in this group. In the study group, the cuffs were inflated using the ‘minimum occlusion’ technique. The mean intracuff pressure measured in the study group was 118.9 mmHg (SD = 54.3). The authors also describe that the use of an endotracheal tube causes mucosal damage at two main sites: the posterior larynx and the anterior and lateral aspect of the trachea between the third and tenth rings. The authors state, “The standard endotracheal tube acts as a curved lever and the posterior larynx, especially the arytenoid and cricoid acts, as a fulcrum 2 when the tube is introduced into the trachea.” They also point out even a relatively short period of endotracheal intubation can result in vocal cord paralysis and tracheal stenosis.
Unlike the external aspects of the patients’ pressure points, damage to the trachea from the ETT and inappropriate cuff pressure cannot be seen. It is important for anesthesia providers to be aware of the physiologic changes that can take place with tracheal intubation and high cuff pressures. Nordin (1977) studied rabbit tracheas due to their similarity in lateral wall anatomy and found progressive damage to the tracheal wall in relation to time and cuff pressure. The
introduction of the endotracheal tube itself created superficial damage and inflation of the cuff resulted in progressive extension of the mucosal damage. A cuff-tracheal (C-T) pressure of 50 mmHg for 2 hours of intubation destroyed most of the epithelial cells on top of the cartilages, and 4 hours of intubation with C-T pressure of 100 could destroy the mucosa down to the cartilage and basement membrane. Bacteria were also found to be invading the damaged mucosa.12
An old belief is that ischemic tracheal injury can occur only with prolonged intubation. Dedo,3 Somri,13 Raynham14 and Rokamp4 all report damage within 15 to 30 minutes of cuff pressure exceeding the tracheal perfusion pressure. According to Dedo3, over-inflation of the ETT cuff for even a brief operation can lead to tracheal stenosis within 1 to 3 months. Additionally, hypovolemia, acidosis, hypoxia and anemia could cause even greater compromise.3
Tracheal stenosis can occur anywhere the endotracheal tube is in contact with the tracheal wall, but most common site is where the ETT cuff has been in contact. In a retrospective review of 31 patients with post intubation (PI) and post tracheostomy (PT) stenosis, Zias15 found the most common profile to be female (73%) obese (66%), history of diabetes (35%), hypertension (52%), cardiovascular disease (45%) and a current smoker (39%). Eleven patients in the PI group had only oro-tracheal intubation (5.2 days mean intubation time) and developed web-like stenosis at the cuff site. All of the comorbidities in the profile would diminish tracheal perfusion even more extensively in the presence of high cuff pressure.
Studies that examine the size of tracheas and endotracheal tube complications support using smaller ETTs. Randestad,16 in an effort to aide transplantation, stenting, intubation, cricothyroidectomy and endoscopic procedures, measured the dimensions of the cricoid cartilage and trachea. A total of 1861 measurements were taken from 34 male and 27 female patients. The longitudinal axes of the cricoaryenoid joint facets ranged from 42 to 74 degrees in women and 37 to 75 degrees in men. The authors concluded that “in some women, the inner diameter of the female cricoid ring does not permit passage of a standard size (7 mm) tracheal tube in some women, and the small distance between the cricoarytenoid joints and standard size tubes cause pressure necrosis at the medial sites of the arytenoid cartilages.”16 Randestad also points out there is a need for better-fitting tubes to avoid unnecessary hoarseness and laryngeal pain.
The tracheal diameter measurements of men and women and the inner diameter (ID) and outer diameter (OD) measurements of ETTs are provided in the table below. It is readily apparent that a size 7.0 diameter ETT with an OD of 9.6 is clearly too large to fit some women. Measurements of trachea from Randestad: Women 8.9 to 17 mm and men 11-21.5 mm.
| Diameter | Size | ID | OD |
|---|---|---|---|
| F 8.9 (smallest) | 6.0 | 6.0 | 8.2 |
| 6.5 | 6.5 | 8.9 | |
| 7.0 | 7.0 | 9.6 | |
| 7.5 | 7.0 | 10.2 | |
| M 11 (smallest) | 8.0 | 8.0 | 10.9 |
Many studies conclude that women are more prone to POST/PH than men.17-20 Jaennsson21 (2012) however, in a prospective cross-sectional study examined risk factors for airway symptoms post-operatively and gender differences and found no significant differences. A total of 495 patients were included with a total of 31 variables. Women were intubated with a size 6.0-7.0 ETT and men with 7.0-8.0 ETT. The main risk factor found for women was ETT size 7.0 and multiple laryngoscopies. For men, the main risk factors were intubation by personnel with < 3 months experience. The main risk factor for hoarseness for both men and women was cuff pressure.
In a study to examine ETT size and sore throat following surgery, Jaensson 22 (2009) looked at 100 healthy women and allocated either a size 6.0 or 7.0 ETT. Post-operatively sore throat and discomfort were assessed at 1-2 hours and 24 hours after extubation. Cuff pressure of the ETTs was measured and maintained at 20-30 cm H2O pressure. The severity of sore throat in the PACU was significantly greater in the ETT 7.0 (38.8%) compared with the ETT 6.0 (18.8%). The grading for throat discomfort was mild to severe for size 7.0 and mild to moderate in the 6.0 ETT group. There were no statistically significant differences between the two groups after PACU. The authors concluded that use of ETT size 6.0 reduces sore throat and discomfort in the early post-operative period.21
Al-Qahtani2 also studied ETT size and incidence of sore throat. A total of 1,618 patients, (883 males and 735 females) were included between February 2000 and May 2003. Size 7.0-7.5 mm cuffed tracheal tubes were used for men and size 6.0-6.5 mm in females. The age group was between 16-62 yrs. and all presented for nasal surgery and/or functional endoscopic sinus surgery. Patients who had signs of common cold were excluded. The authors found that the use of small tube in intubating the trachea, together with other measures (lubricating, careful instrumentation, intubating only when fully relaxed and extubating when the cuff was fully deflated), have dramatic effects on minimizing the incidence of postoperative sore throats.
As pointed out for cuff pressure damage, anesthesia providers are unable to see the physiologic changes associated with large endotracheal tubes. It is described by Dedo in his book Surgery of the Larynx and Trachea “… the mucosa and the perichondrium of the arytenoid cartilages can be necrosed by an endotracheal tube that is too large….If the endotracheal tube pressure causes the necrosis to extend into the cricoarytenoid joints, they will become frozen, so
that even if posterior commissure stenosis is repaired, the vocal cords will not be able to adduct (open) to provide an adequate airway.”3
Vocal cord injury and hoarseness are clinically relevant complications related to shortterm general anesthesia and an endotracheal tube.23 Vocal cord paralysis is secondary to damage to the recurrent laryngeal nerve (RLN) and may occur because the endotracheal tube cuff presses the recurrent laryngeal nerve between the thyroid lamina and the arytenoid cartilage.24,25
Cros24 described two cases, one permanent, of unilateral RLN palsy following brief periods of intubation. The author concluded that the cause of paralysis was a compression of the nerve between the endotracheal tube cuff and cricoid or from compression between the thyroid ala and a dislocated artenoid cartilage from an unnecessarily large tube.
Otani26 documented nerve palsy in four patients after surgery with an endotracheal tube. The explanation offered was excessive pressure for the inflated ETT on the intralaryngeal course of the anterior branch of the RLN. The authors also concluded monitoring cuff pressure is most important in preventing these nerve injuries. Brandwein25 describes a bilateral vocal cord paralysis following endotracheal intubation and stated the anterior ramus of the RLN is particularly vulnerable to compression injury
Although some of the preceding studies were from older case studies, the problem still exists today. In 2012, Mendels23 performed a literature review to determine the occurrence and type of vocal cord injury and hoarseness in adults using an ETT in short-term anesthesia (<5 hours). Thirteen studies met the inclusion criteria. After analysis of the studies, the authors concluded hoarseness and vocal cord injuries were common after short-term anesthesia and
lasted up to 6 months. The authors found the following risk factors of laryngeal injury caused by an ET: direct intubation trauma or tracheal extubation, ET size, cuff design, cuff pressure, type of tube, use of an introducer, use of a gastric tube, muscle relaxation, use of propofol, duration of the operation, intubation conditions, and movement of the tube, as well as demographic factors such as sex, weight, history of smoking and gastroesophageal reflux. The limitation of the study is that the authors reviewed were heterogeneous and, therefore, hard to compare.
Verhagen27 describes an 80-year-old man who sustained left RLN palsy after total hip arthroplasty. The two theories for cause were either an injury from the intubation or a stretch injury from positioning. Whichever the cause, it demonstrates we need to be concerned with the tracheal nerves just as we are with the extremities.
Discussion:
The studies that were discussed in this paper make clear that clinicians have poor ability to properly inflate cuffs to safe pressures without a cuff manometer.28 As stated before, an ETTc pressure lower than 20 cm H2O pressure places the patient at risk of micro-aspiration and pneumonia19 and a pressure higher than 30 cm H2O places the patient at risk of tracheal ischemia, necrosis and stenosis.12,28,29 Wujtewizc7 found cuff pressures frequently exceed safe limits. It is imperative to maintain the cuff pressure of 20-30 cm H2O. Wujtewicz,7 Chen,19 Hoffman,2 Stridermma,30 Watson31 and Braz29 all suggest routine measurement and control of ETT cuff pressure with a cuff manometer to maintain cuff pressure between 20-30 cm H2O.
It is unclear where the standardized sizes of 7.0 ETT for females and 8.0 ETT for men originated. Exhaustive literature searches have not revealed the reasoning behind these sizes. Stoelting and Miller, in their book Basics of Anesthesia (3rd edition), state, “Most adult tracheas (after 14 years of age) readily accept a cuffed 8- to 9- mm ID (smaller size often selected for females) tracheal tubes.”32 No supporting evidence or references were provided for their sizing choices. One hypothesis of adult ETT sizing is that when endotracheal tubes were first introduced, they did not have pilot balloons, requiring large sizes to prevent air and gas leaks and to provide adequate ventilation. Larger sizes were then handed down as routine practices. As 5 stated before, this is just a hypothesis and cannot be proven. Similarly, the reasoning for the historical standard sizes of 7.0 for women and 8.0 for men remains hidden.
Work of breathing (WOB) is frequently cited as the rationale for choosing larger size tubes. Fiastro33 disputed this in 1988 with the conclusion that pressure support can be used to compensate for the added inspiratory work due to artificial airway resistance. In 1998 Koh34 discussed WOB, and found positive pressure ventilation could be achieved with the use of small sizes of tracheal tubes and that there is evidence that glottis damage is less likely when smaller
sizes of tube are used.
To improve patient safety and prevent life altering complications like subglottic tracheal stenosis, it is imperative to downsize routine adult endotracheal tubes and to check the cuff pressure with a manometer with each and every intubation.